Nurse practitioner chart review requirements are one of the clearest examples of how state-by-state collaboration law shapes real clinical operations. For healthcare organizations that employ or contract with NPs across multiple states, it can be challenging to knowing when chart review applies, how often it must happen, how it should be documented, and how those rules change as NPs move through transition-to-independence pathways.
NP collaboration rules create an operational spectrum shaped by collaboration type, physician involvement, recurring oversight tasks, and transition thresholds.
This article explains how NP chart review requirements work across the United States, what healthcare organizations need to watch for, and how to build an oversight process that can hold up as your NP workforce grows.
Note: This article is a strategic operational guide, not legal advice. Organizations should still confirm current statutes, board rules, and specialty-specific requirements for the most up-to-date information.
Key Takeaways
- NP chart review requirements vary widely by state and do not fit neatly into one national standard.
- Some states do not require ongoing physician collaboration at all, while others require monthly, quarterly, annual, or state-defined quality assurance activity.
- In many states, chart review is tied to broader collaboration compliance, which can also include meetings, quality assurance plans, board filings, and documentation retention.
- Transition states matter. An NP may begin practice under one set of chart review rules and later move to reduced oversight or independence after a required number of hours or years.
- Healthcare organizations need a state-specific operating model, not a one-size-fits-all policy, if they want to stay compliant and scale responsibly.
What Are NP Chart Review Requirements?
NP chart review requirements are state-driven oversight rules that define whether a collaborating physician must review some portion of an NP’s clinical work and, if so, how often that review must happen.
In practice, “chart review” can mean different things in different states. It may involve:
- A fixed monthly or weekly review cadence
- A quarterly or annual review requirement
- A required quality assurance process rather than a set percentage
- A review requirement tied only to prescribing, such as controlled substances
- No formal chart review requirement at all
That variation is exactly why chart review creates operational problems for multi-state healthcare organizations.
Why State-by-State Chart Review Rules Matter
NP chart review affects staffing, physician capacity, onboarding speed, compliance risk, and clinical quality workflows.
Most states that require collaboration also impose ongoing compliance tasks after a collaboration agreement is signed. These often include periodic chart review, meetings between the NP and physician, documented quality assurance processes, monitoring of physician-to-NP ratios, and updates when prescriptive authority or practice sites change.
That means chart review is rarely a standalone task. It is usually part of a broader collaboration compliance program.
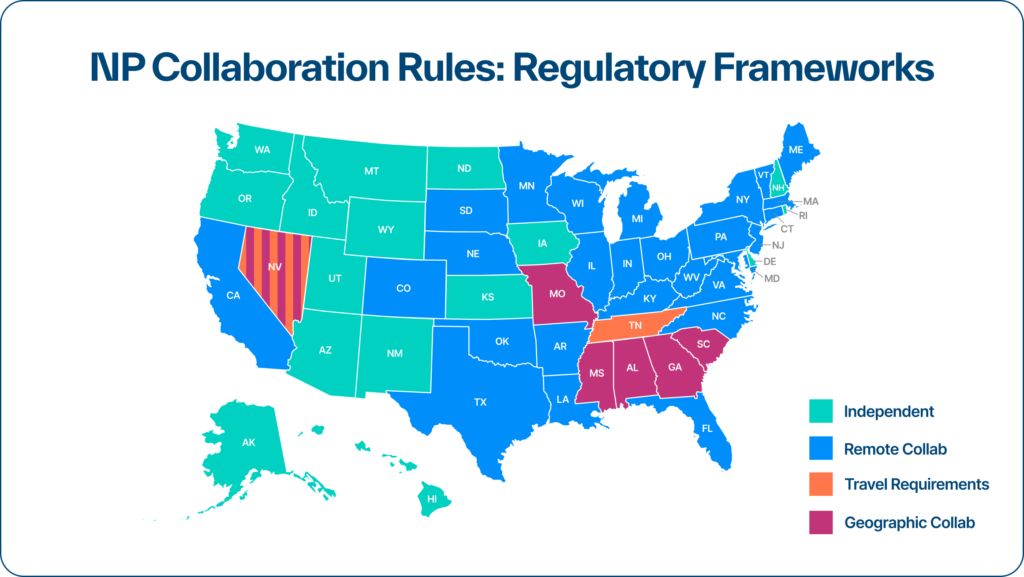
Chart Review Models: Regulatory Frameworks
Before getting into the state-by-state guide, it helps to define the basic regulatory buckets.
Independent States
These are states where NPs may practice independently without a standing physician collaboration requirement. In those states, there is generally no state-mandated NP chart review requirement tied to collaboration law, though employers, payers, malpractice carriers, or internal quality programs may still require review. Zivian’s guide shows that many states fall into this category for NPs.
Remote Collaboration States
These states require a physician relationship, but do not impose ongoing geographic restrictions on where the physician is physically located. The oversight requirements still vary widely. Some remote collaboration states have low physician involvement, while others require monthly, quarterly, or annual chart review or QA activity.
Geographic or Travel Requirement States
These states require more direct physical involvement. In some, the physician must be on site at defined intervals, located in state, or meet other geographic expectations. These states often carry the highest operational burden.
Transition States
These states reduce oversight after the NP completes a set number of clinical hours or years in practice. Some transition states lead to full independence. Others only reduce the intensity of oversight while keeping collaboration in place.
Employers should remain aware of transition state thresholds, because the rules at hire may not be the rules that apply a year or two later.
What Counts as “Chart Review” in State Law?
State law does not always use consistent language for chart review. Depending on the state, you may see the requirement framed as:
- Chart review
- Quality assurance review
- Periodic review
- A meaningful sample review
- A prescribing-only review
- A broader QA process without a fixed chart percentage
That matters, because an organization can miss the requirement if it searches only for the phrase “chart review.”
Chart review is part of ongoing collaboration compliance and recurring oversight can include chart review, meetings, documented QA processes, and other recurring records that must be tracked over time.
State-by-State NP Chart Review Requirements
Below is a state-by-state summary of NP chart review requirements. This section focuses on collaboration-driven chart review and related oversight requirements for NPs.
States where NPs are generally independent
These states generally offer independent practice for NPs, meaning there is no standing physician collaboration requirement under the framework and therefore no ongoing chart review requirement tied to the collaboration model:
- Alaska
- Arizona
- District of Columbia
- Delaware
- Hawaii
- Idaho
- Iowa
- Kansas
- Montana
- New Hampshire
- New Mexico
- North Dakota
- Oregon
- Rhode Island
- Utah
- Washington
- Wyoming
For healthcare organizations, this does not mean “no oversight ever.” It means the state does not impose an ongoing collaboration-based chart review structure in the same way restricted or reduced practice states do.
States where QA or chart review is required, but defined more broadly
Several states require review or QA activity without framing it as a simple monthly percentage rule. Examples include:
- Alabama: QA required with quarterly meetings in a geographic model
- Arkansas: QA required and QA-required meetings in a remote collaboration model
- California: QA required and QA-required meetings in a remote model during transition phases
- Connecticut: QA required and QA-required meetings in a remote model during transition phases
- Massachusetts: QA required and QA-required meetings; collaboration for prescriptive practice only during transition structure noted separately
- Vermont: QA required and QA-required meetings in its transition model
These states often require more than a spreadsheet checkbox. They require a defined QA workflow.
States with periodic, annual, or state-defined review language
Some states set lower-frequency or more flexible review language:
- Illinois: “periodically,” with Schedule II-only meetings; transition state
- New Jersey: “periodically”
- New York: quarterly review in its transition structure
- Ohio: annual chart review and annual meetings
- Oklahoma: chart review “appropriately” and meetings “regularly”; prescribing-only collaboration carve-out noted in transition rules
- West Virginia: annual chart review and annual meetings
These states may look lower burden on paper, but vague language can create its own compliance risk if the organization has no defined standard.
States with higher-burden recurring chart review requirements
These states are among the most operationally demanding because they call for recurring chart review or QA activity on a regular cadence:
- Indiana: weekly chart review
- Missouri: bi-weekly chart review and bi-weekly meetings; prescribing-only vicarious liability noted in the guide
- Georgia: monthly chart review and annual meetings in a geographic model
- Mississippi: monthly chart review and quarterly meetings in a geographic model; controlled substance prescribing liability for collaborating physician
- North Carolina: monthly chart review plus QA-required meetings
- Tennessee: monthly chart review and monthly meetings in a travel-requirement model; controlled substance prescribing liability for collaborating physician
- Texas: required chart review and monthly meetings
- Nevada: required chart review plus monthly on-site QA in its pre-transition model
These are the states most likely to break a manual process first.
Quick-Reference: NP Chart Review Rules by State
Here is a concise operational reference for every state in the U.S.
- Alabama: Geographic collaboration; high physician involvement; QA required; quarterly meetings. Transition state.
- Alaska: Independent.
- Arizona: Independent.
- Arkansas: Remote collaboration; standard involvement; QA required; QA-required meetings. Transition state.
- California: Remote collaboration; standard involvement; QA required; QA-required meetings. Transition state.
- Colorado: Remote collaboration; low involvement; no chart review listed in the table. Transition state.
- Connecticut: Remote collaboration; standard involvement; QA required; QA-required meetings. Transition state.
- District of Columbia: Independent.
- Delaware: Independent.
- Florida: Remote collaboration; low involvement; no chart review listed in the table. Transition state.
- Georgia: Geographic collaboration; high involvement; monthly chart review; annual meetings.
- Hawaii: Independent.
- Idaho: Independent.
Illinois: Remote collaboration; standard involvement; chart review “periodically.” Transition state. - Indiana: Remote collaboration; high involvement; weekly chart review.
- Iowa: Independent.
- Kansas: Independent.
- Kentucky: Remote collaboration; low involvement; controlled-only oversight note in the table. Transition state.
- Louisiana: Remote collaboration; low involvement; no chart review listed in the table.
- Maine: Remote collaboration; low involvement; no chart review listed in the table. Transition state.
- Maryland: Remote collaboration; low involvement; no chart review listed in the table. Transition state.
- Massachusetts: Remote collaboration; standard involvement; QA required; QA-required meetings. Transition state.
- Michigan: Remote collaboration; low involvement; no chart review listed in the table.
- Minnesota: Remote collaboration; low involvement; no chart review listed in the table. Transition state.
- Mississippi: Geographic collaboration; high involvement; monthly chart review; quarterly meetings. Transition state.
- Missouri: Geographic collaboration; high involvement; bi-weekly chart review; bi-weekly meetings. Prescribing-only vicarious liability noted.
- Montana: Independent.
- Nebraska: Remote collaboration; low involvement; no chart review listed in the table. Transition state.
- Nevada: Geographic/travel model; high involvement; required chart review; monthly on-site QA. Transition state.
- New Hampshire: Independent.
- New Jersey: Remote collaboration; standard involvement; chart review “periodically.”
- New Mexico: Independent.
- New York: Remote collaboration; standard involvement; quarterly chart review in current transition model. Transition state. Zivian also notes a major 2026 change discussed below.
- North Carolina — Remote collaboration; high involvement; monthly chart review; QA-required meetings.
- North Dakota: Independent.
- Ohio: Remote collaboration; standard involvement; annual chart review; annual meetings.
- Oklahoma: Remote collaboration; standard involvement; chart review “appropriately”; meetings “regularly.” Transition state with prescribing carve-out.
- Oregon: Independent.
- Pennsylvania: Remote collaboration; standard involvement; chart review required; physician must be available.
- Rhode Island: Independent.
- South Carolina: Geographic collaboration; low involvement; no chart review listed in the table.
- South Dakota: Remote collaboration; low involvement; no chart review listed in the table. Transition state.
- Tennessee: Travel requirement model; high involvement; monthly chart review; monthly meetings. Transition state.
- Texas: Remote collaboration; high involvement; chart review required; monthly meetings.
- Utah: Independent.
- Vermont: Remote collaboration; standard involvement; QA required; QA-required meetings. Transition state.
- Virginia: Remote collaboration; standard involvement; chart review required. Transition state.
- Washington: Independent.
- West Virginia: Remote collaboration; standard involvement; annual chart review; annual meetings. Transition state.
- Wisconsin: Remote collaboration; low involvement; no chart review listed in the table. Transition state, with future independent pathway discussed below.
- Wyoming: Independent.
NP Transition States: Why They Matter for Chart Review Compliance
Transition states deserve special attention because chart review requirements can change over time.
Many transition states move NPs from a more structured collaboration model to a lower-burden model or full independence after a required number of hours or years. Examples include:
- Colorado: 750 hours to independence, where collaboration is only required if provisional prescriptive authority is granted
- Connecticut: 2,000 hours to independence
- Florida: 3,000 hours to independence, but only for certain primary care categories; aesthetics has added restrictions before transition
- Illinois: 4,000 hours to independence
- Minnesota: 2,080 hours to independence
- New York: 3,600 hours currently transition the NP to a lower-burden remote model, but this changes in 2026
- Oklahoma: 6,240 hours to independence, but Schedule II prescribing still requires collaboration
- Virginia: 5,400 hours to independence
- West Virginia: 3 years to independence, but collaboration is required for prescribing only
- Wisconsin: 3,840 hours to independence
The takeaway is simple: your chart review workflow should be tied to the NP’s current regulatory stage, not just the state name.
Common Compliance Mistakes Organizations Make
Treating all chart review requirements as monthly
Some states are monthly, some are weekly, some are annual, some say QA required, and some are independent.
If you assume a national monthly rule, you will overbuild in some places and miss obligations in others.
Tracking only the collaboration agreement
The agreement is just the beginning. Ongoing collaboration compliance often includes recurring chart review, meetings, QA processes, ratio monitoring, renewals, and change documentation.
Missing the transition event
If an NP reaches a threshold for reduced oversight or independence and your organization does not update its process, you can either create unnecessary admin burden or fail to shift to the right legal model.
Ignoring prescribing carve-outs
Some states require continued collaboration for controlled substances or specific schedules even after the NP reaches an independence threshold. Oklahoma, Kentucky, Nevada, West Virginia, and other states show why organizations need to separate general practice status from prescribing status.
How to Build a State-Specific NP Chart Review Program
A scalable program usually includes five core elements:
- A current state rules inventory: Keep a live record of chart review, meeting, QA, filing, and prescribing rules by state.
- A provider-level status view: Track whether each NP is in a pre-transition, post-transition, or independent status.
- A standard review workflow: Use consistent templates, role-based assignments, due dates, and documentation rules.
- An audit trail: Preserve evidence of chart selection, review completion, findings, meeting attestations, and agreement updates.
- A change-management process: Update workflows when state law changes, when NPs gain hours, or when prescribing scope changes.
This is where many organizations feel the difference between a policy and an operating system.
Why Chart Review Is Also a Clinical Quality Issue
Chart review is often discussed as a compliance task, but it also creates clinical quality data.
When healthcare organizations standardize chart review well, they can use the process to:
- Identify recurring documentation issues
- Track prescribing and referral patterns
- Support NP development
- Surface quality trends across service lines or states
- Give clinical leaders a more reliable view of performance
Chart review is both a compliance signal and a clinical quality signal. Ongoing oversight is presented as part of the infrastructure required to operationalize APP-integrated care responsibly at scale.
How Zivian Helps Healthcare Organizations Manage Chart Review and Clinical Quality
Zivian helps healthcare organizations manage the operational complexity behind NP collaboration compliance and clinical quality oversight. The Zivian platform is designed to support agreement execution, ongoing compliance tracking, regulatory monitoring, and centralized visibility across the states where an organization operates.
Zivian translates nuanced regulations into structured workflows so that healthcare enterprises can activate clinicians faster, maintain consistent oversight, and manage recurring requirements at scale.
Interested in simplifying your compliance operations? Connect with us today to get started.